FDA Overhaul Needed for New Vaccines and mRNA Therapies
The pandemic is over, but the introduction of COVID-19 vaccines that use mRNA technology marks the beginning of a new era in modern medicine. The FDA’s haphazard regulatory framework for mRNA vaccine approval has set the stage for adverse events related to genetic therapies using this new technology. As public documents are released, we will reveal emerging concerns about mRNA injections related to lipid nanoparticles, spike protein, and vaccine contamination in this series.
Summary of Series Key Facts
Moderna filed a Securities and Exchange Commission filing in June 2020, stating that “currently, mRNA is considered a gene therapy product by the Food and Drug Administration (FDA).”
The FDA issued new guidance in June 2020 for gene therapy products to be marketed as COVID-19 vaccines. They were not subjected to the same rigorous testing as other RNA therapeutics. The new vaccines were also exempt from human biodistribution studies.
If mRNA vaccines had been subjected to the same regulatory scrutiny as novel therapeutics, the following three issues would almost certainly have been identified prior to human use:
The lipid nanoparticle (LNP) shell used to deliver the mRNA has inflammatory potential and can cluster with other LNPs or fall apart, allowing the mRNA inside to fall out and freely circulate in the bloodstream.
Following vaccination, the spike protein encoded by the mRNA and its S1 subunit was discovered in the blood. The spike protein and the S1 subunit are both involved in inflammation and clotting.
Impurities in the vaccine, such as mRNA fragments and bacterial plasmids, can be caused by contamination during the manufacturing process. Impurities were discovered during pharma testing prior to approval; have these issues been resolved?
- Despite the promising potential of mRNA therapeutics, did the COVID-19 pandemic emergency justify the suspension of standard regulatory requirements?
- Should these vaccines have been recommended only for the most vulnerable people, pending further human testing? Should all known risks have been included in vaccine information sheets to allow for full and complete informed consent?
- Given the lack of standard pre-authorization safety testing, were mandates unethical?
- Given the development of new mRNA vaccines against influenza and respiratory syncytial virus, all of these questions are pertinent. What regulatory framework will be used in the future? Will these newer mRNA vaccines be subjected to stricter oversight aligned with, to use Moderna’s terminology, “genetic therapy” or the lagging framework used for COVID-19 mRNA vaccines?
When a new vaccine for humans is developed, it is subjected to extensive safety testing, first in animals, then in humans. That’s how it usually goes. An analogy will be useful in explaining what happened with the mRNA vaccines. Assume the COVID-19 vaccine was the first bioengineered egg approved by the FDA for human consumption. The “shell” of the egg is the LNP capsule, which contains the genetically modified “contents,” mRNA and spike protein.
The FDA decided to relax its regulations and test only the LNP shell in animals, omitting testing of the contents (mRNA and spike protein) in animals or humans. This testing (biodistribution study) would have determined how the body reacts to the new technology.
In other words, the FDA approved the first-ever mRNA “vaccine” to be injected into a human body without first assessing the biodistribution of the “contents” (mRNA and spike protein) for human safety. It only examined the LNP “shell” on animals before stamping its approval. Even the limited data on LNP testing is concerning.
Despite the lack of adequate safety testing for the first mRNA “vaccine” used in humans, the FDA granted approval and assured the public that the entire product was safe. As serious adverse events occurred at an unprecedented rate, the FDA increased its safety claims, requiring no additional research.
The limited data we have is concerning because it shows that the LNP spreads throughout the body rather than remaining in one location. This level of testing is not allowed for the approval of other drugs.
The European Medicines Agency (EMA), the European equivalent of the US FDA, was more open than the FDA in terms of the limited data available. The EMA provided numerous details regarding how the LNP (the “shell”) spreads throughout the body. It was also concerned about impurities in vaccines during manufacturing. This series will go over these topics in depth, including excerpts from EMA reports. The Pfizer report to the FDA, which we will also discuss, was only made available after a Freedom of Information Act request, which is a legal mechanism for compelling disclosure. Why is it so difficult to share testing data?
Relaxed Regulations for COVID mRNA Vaccines
A health authority must understand how the body will process a new drug or vaccine before it can be approved.
A nonclinical pharmacokinetics study report is typically submitted to the FDA in order to explain how the drug is released, absorbed, distributed, metabolized, and excreted from the body. This is referred to as a biodistribution study.
During the COVID-19 pandemic, however, the FDA modified its standard approval process for new vaccines in response to the public health emergency. In June 2020, the pharmaceutical industry received new “nonbinding recommendations” that relaxed the rules for mRNA vaccine approval in comparison to what is typically required for “gene therapy.”
The new FDA guidance, “Development and Licensure of Vaccines to Prevent COVID-19,” permitted companies to present data gathered from other development platforms. In other words, studies on other products were allowed to be used to support the mRNA vaccines’ application for emergency use:
“COVID-19 vaccine development may be accelerated based on knowledge gained from similar products manufactured with the same well-characterized platform technology, to the extent legally and scientifically permissible.”
Nonclinical safety studies may not be required prior to FIH [first in human] clinical trials in some cases because adequate information to characterize product safety may be available from other sources. For example, if the COVID-19 vaccine candidate is made using a platform technology previously used to manufacture a licensed vaccine or other previously studied investigational vaccines and is sufficiently characterized, toxicology data (e.g., data from repeat dose toxicity studies, biodistribution studies) and clinical data accrued with other products made using the same platform may be used to support FIH clinical trials for that COVID-19 vaccine candidate.” The request for biodistribution studies is written in broad strokes, with insufficient specificity for a novel therapeutic like COVID-19 mRNA vaccines:
“If the vaccine construct is novel in nature and there is no existing biodistribution data from the platform technology, biodistribution studies in an animal species should be considered.” If there is a possibility of altered infectivity and tissue tropism, or if a novel route of administration and formulation is to be used, these studies should be carried out.”
While the FDA approved these products under these lax rules, other scientists believe that more specificity is required. According to mRNA researcher Pieter Vervaeke and colleagues, “the rapid rise of mRNA therapeutics has resulted in a regulatory framework that is somewhat lagging.” In the abstract, they go on to say that a “multi-layered approach” should be used to figure out what the new products do in vivo (in the human body).
“Biodistribution studies for RNA therapeutics should encompass both the RNA molecule(s), the individual components of the carrier, the combined RNA-carrier drug, and the produced protein,” the researchers wrote.
In other words, examine both the shell and the contents of the egg.
As we will show, following such guidelines would have been extremely beneficial prior to human use authorization. However, none of the current COVID-19 mRNA vaccines have been subjected to such biodistribution studies in order to evaluate the RNA molecule and its encoded spike protein. Only the LNP carrier capsule has been studied in this way, and it has only been done in animals, not humans.
FDA Review of Pfizer Biodistribution Study
In November 2020, the FDA reviewed Pfizer’s BNT162b2 LNP carrier biodistribution study report based on the FDA’s modified rules for mRNA vaccines to understand how the mRNA vaccine would work. On November 9, 2020, the report was marked as “approved” (pdf).
This report was widely adopted by the European Medicines Agency, the Australian Therapeutic Goods Administration, and the Japanese government, as will be shown in Parts 1 and 2.
The LNP, on the other hand, is only the carrier of the vaccine mRNA (the “shell” of the “egg”), not the main active ingredient of the mRNA vaccine (the contents of the “egg”).
The inside of the “egg” was replaced with a different mRNA—the mRNA carried in the LNP study was coded for luciferase rather than the spike-protein encoding mRNA used in the vaccine. Finally, two of the lipids used in the LNP molecule were not previously approved for human use. As a result, while novel lipids were being developed to carry a novel vaccine for a mass vaccination campaign, no human biodistribution studies were requested.
Human studies are typically required early in drug development by the FDA, and as few as six healthy volunteers would have been required. Given that our bodies produce the spike protein after the vaccine is injected, human studies on the production, distribution, and metabolism of the mRNA and spike protein throughout the body should have been conducted.
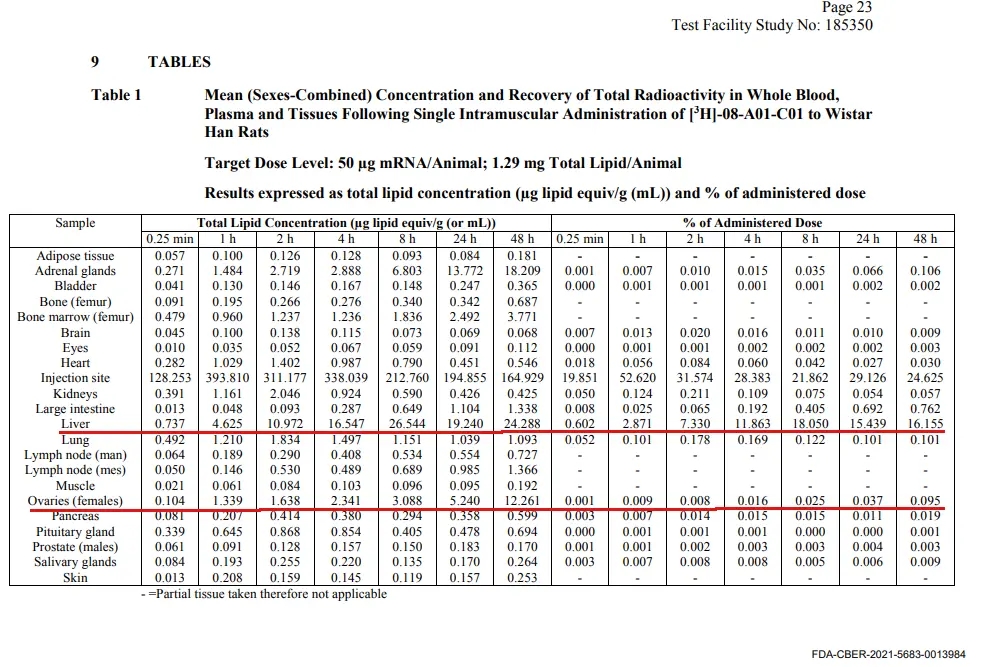
Animal studies, while not ideal, do provide useful information. Pfizer’s biodistribution study report used radioactive labeling to tag the LNPs in the vaccine given to 21 male and 21 female rats. This enabled the researchers to track and quantify the amount of vaccine reaching various organs 48 hours after injection.
The rats were given 50 micrograms of mRNA vaccine. In addition to having a relatively high mRNA concentration at the injection site after 15 minutes, the vaccine began to disperse to different organs throughout the body, with the liver and spleen being the first to be reached.
After an hour, the vaccine concentration in the liver and spleen increased even more, and it reached the adrenal glands and bone marrow.
After 24 hours, the researchers examined the distribution of the mRNA vaccine in the rats and discovered that, in order of concentration, the highest levels were in the spleen, liver, adrenal glands, ovaries, bone marrow, lymph nodes, kidneys, muscles, and heart. At 48 hours, the liver reading was 24.288. This figure appears in both the Australian and Japanese reports, which will be covered in Part 2 of this series.
Figure 1: Rat Biodistribution Study Data in an FDA Report
CDC’s Silent Removal of Reassuring Message
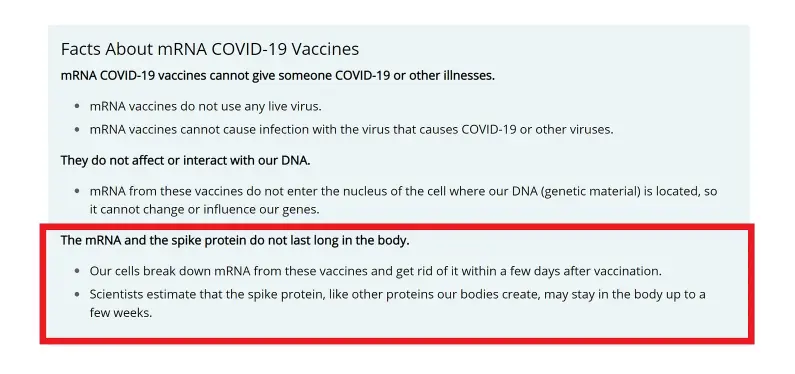
Following approval, the Centers for Disease Control and Prevention (CDC) sought to allay concerns about toxicity by claiming that the mRNA is quickly broken down and removed from the body, whereas the spike protein may take longer.
However, these claims (see below in red box), which appeared on the CDC website on July 15, 2022, have been quietly removed. Is the CDC thus acknowledging that evidence to support these claims is lacking?
Figure 2a: The CDC Assures Us That mRNA and Spike Protein Disintegrate Rapidly
The CDC updated this web page sometime after July 2022 to reassure the public that the mRNA vaccine does not integrate into the human genome, with no mention of how long the spike protein and mRNA will remain in the body.
Figure 2b: CDC Reassurance That mRNA Doesn’t Enter the Cell Nucleus
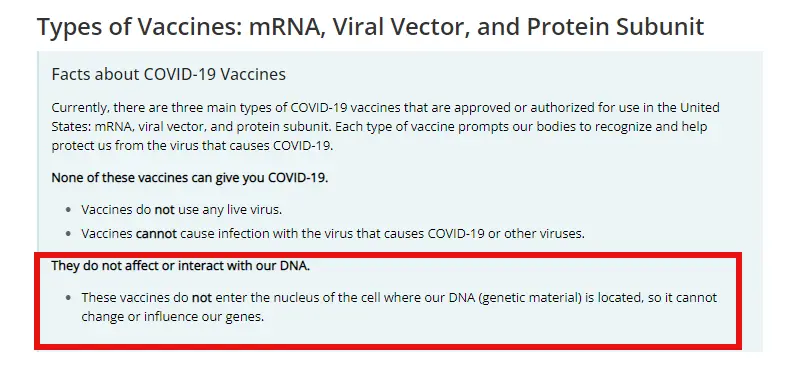
Why did the CDC change its website messaging to emphasize DNA integration rather than how long mRNA and spike protein last in the body?
Next: A closer look at reports from health authorities in Australia, Japan, and Europe explains why the CDC may have withdrawn the claim that mRNA is quickly broken down and spike protein does not linger in the body. The EMA reports show the path of the LNP shell and mRNA throughout the body.
◇ References
Addgene. Molecular Biology Reference.
Alana F Ogata, Chi-An Cheng, Michaël Desjardins, Yasmeen Senussi, Amy C Sherman, Megan Powell, Lewis Novack, Salena Von, Xiaofang Li, Lindsey R Baden, David R Walt, Circulating Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients, Clinical Infectious Diseases, Volume 74, Issue 4, 15 February 2022, Pages 715–718.
Aldén M, Olofsson Falla F, Yang D, Barghouth M, Luan C, Rasmussen M, De Marinis Y. Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line. Curr Issues Mol Biol. 2022 Feb 25;44(3):1115-1126. doi: 10.3390/cimb44030073. PMID: 35723296; PMCID: PMC8946961.
Anderson EJ, Rouphael NG, Widge AT, et al. Safety and Immunogenicity of SARS-CoV-2 mRNA-1273 Vaccine in Older Adults N Engl J Med 2020; 383:2427-2438
Anderson S. CBER Plans for Monitoring COVID-19 Vaccine Safety and Effectiveness. October 20, 2020. Accessed 3/20/23.
Angeli F, Spanevello A, Reboldi G, Visca D, Verdecchia P. SARS-CoV-2 vaccines: Lights and shadows. Eur J Intern Med. 2021 Jun;88:1-8. doi: 10.1016/j.ejim.2021.04.019. Epub 2021 Apr 30. PMID: 33966930; PMCID: PMC8084611.
Baker, A. T., Boyd, R. J., Sarkar, D., Teijeira-Crespo, A., Chan, C. K., Bates, E., Waraich, K., Vant, J., Wilson, E., Truong, C. D., Lipka-Lloyd, M., Fromme, P., Vermaas, J., Williams, D., Machiesky, L., Heurich, M., Nagalo, B. M., Coughlan, L., Umlauf, S., Chiu, P. L., … Borad, M. J. (2021). ChAdOx1 interacts with CAR and PF4 with implications for thrombosis with thrombocytopenia syndrome. Science Advances. 7(49), eabl8213.
Baumeier C, Aleshcheva G, Harms D, Gross U, Hamm C, Assmus B, Westenfeld R, Kelm M, Rammos S, Wenzel P, Münzel T, Elsässer A, Gailani M, Perings C, Bourakkadi A, Flesch M, Kempf T, Bauersachs J, Escher F, Schultheiss H-P. Intramyocardial Inflammation after COVID-19 Vaccination: An Endomyocardial Biopsy-Proven Case Series. International Journal of Molecular Sciences. 2022; 23(13):6940.
Bloom, K., van den Berg, F. & Arbuthnot, P. Self-amplifying RNA vaccines for infectious diseases. Gene Ther 28, 117–129 (2021).
Chauhan, H., Mohapatra, S., Munt, D.J. et al. Physical-Chemical Characterization and Formulation Considerations for Solid Lipid Nanoparticles. AAPS PharmSciTech 17, 640–651 (2016).
Chui CSL, Fan M, Wan EYF, et al. Thromboembolic events and hemorrhagic stroke after mRNA (BNT162b2) and inactivated (CoronaVac) covid-19 vaccination: A self-controlled case series study. Lancet. 2022;(50).
Dag Berild J, Bergstad Larsen V, Myrup Thiesson E, et al. Analysis of Thromboembolic and Thrombocytopenic Events After the AZD1222, BNT162b2, and MRNA-1273 COVID-19 Vaccines in 3 Nordic Countries. JAMA Netw Open. 2022;5(6):e2217375. doi:10.1001/jamanetworkopen.2022.17375.
daSilva RL. Viral-associated thrombotic microangiopathies. Hematology/Oncology and Stem Cell Therapy. 2011:4(2):51-59.
De A, Ko YT. Why mRNA-ionizable LNPs formulations are so short-lived: causes and way-out. Expert Opin Drug Deliv. 2023 Feb;20(2):175-187. doi: 10.1080/17425247.2023.2162876. Epub 2023 Jan 1. PMID: 36588456.
Doshi P. BMJ 2021;373:n1244 Covid-19 vaccines: In the rush for regulatory approval, do we need more data? | The BMJ
Ehaideb, S.N., Abdullah, M.L., Abuyassin, B. et al. Evidence of a wide gap between COVID-19 in humans and animal models: a systematic review. Crit Care 24, 594 (2020).
European Medicines Agency Assessment Report
Faizullin D, Valiullina Y, Salnikov V, Zuev Y. Direct interaction of fibrinogen with lipid microparticles modulates clotting kinetics and clot structure. Nanomedicine. 2020 Jan;23:102098. doi: 10.1016/j.nano.2019.102098. Epub 2019 Oct 23. PMID: 31655206.
FDA. Considerations for Human Radiolabeled Mass Balance Studies—Guidance for Industry. May 2022.
FDA. Development and Licensure of Vaccines to Prevent COVID-19.
FDA-CBER-2021-5683-0013962 approved on: 09-Nov-2020. A Tissue Distribution Study of a [3H]-Labeled Lipid Nanoparticle-mRNA Formulation Containing ALC-0315 and ALC-0159 Following Intramuscular Administration in Wistar Han Rats. FINAL REPORT Test Facility Study No. 185350 Sponsor Reference No. ALC-NC-0552
Fertig TE, Chitoiu L, Marta DS, Ionescu VS, Cismasiu VB, Radu E, Angheluta G, Dobre M, Serbanescu A, Hinescu ME, Gherghiceanu M. Vaccine mRNA Can Be Detected in Blood at 15 Days Post-Vaccination. Biomedicines. 2022 Jun 28;10(7):1538. doi: 10.3390/biomedicines10071538. PMID: 35884842; PMCID: PMC9313234.
Grobbelaar LM et al. SARS-CoV-2 spike protein S1 induces fibrin(ogen) resistant to fibrinolysis: implications for microclot formation in COVID-19 Biosci Rep (2021) 41 (8): BSR20210611.
Hou, X., Zaks, T., Langer, R. et al. Lipid nanoparticles for mRNA delivery. Nat Rev Mater 6, 1078–1094 (2021).
Let’s talk about lipid nanoparticles. Nat Rev Mater 6, 99 (2021).
Michieletto, D., Lusic, M., Marenduzzo, D. et al. Physical principles of retroviral integration in the human genome. Nat Commun 10, 575 (2019).
Moghimi, S. M., & Simberg, D. (2022). Pro-inflammatory concerns with lipid nanoparticles. Molecular therapy: The Journal of the American Society of Gene Therapy, 30(6), 2109–2110.
Naturally Inspired Podcast. Jessica Rose Ph.D. VAERS, Data and Truth
Ohlson J. Plasmid manufacture is the bottleneck of the genetic medicine revolution. Drug Discov Today. 2020 Oct 16;25(11):1891–3. doi: 10.1016/j.drudis.2020.09.040. Epub ahead of print. PMID: 33075470; PMCID: PMC7564888.
Perico L, Marina Morigi M, Galbusera M, et al. SARS-CoV-2 Spike Protein 1 Activates Microvascular Endothelial Cells and Complement System Leading to Platelet Aggregation. Front. Immunol. 2022.
Qin, S., Tang, X., Chen, Y. et al. mRNA-based therapeutics: powerful and versatile tools to combat diseases. Sig Transduct Target Ther 7, 166 (2022).
Röltgen K, Nielsen SCA, Silva O. Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination. Cell 2022;185(6):1025-1040.
Schmeling, M, Manniche, V, Hansen, PR. Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine. Eur J Clin Invest. 2023; 00:e13998. doi:10.1111/eci.13998
Srinivasan M, Thangaraj SR, Arzoun H. Gene Therapy – Can it Cure Type 1 Diabetes? Cureus. 2021 Dec 19;13(12):e20516. doi: 10.7759/cureus.20516. PMID: 35004071; PMCID: PMC8723777.
Trougakos IP, Terpos E, Alexopoulos H, et al. Adverse effects of COVID-19 mRNA vaccines: the spike hypothesis. Cell 2022;28(7): P542-554.
Vervaeke P, Borgos SE, Sanders NN, Combes F. Regulatory guidelines and preclinical tools to study the biodistribution of RNA therapeutics. Adv Drug Deliv Rev. 2022 May;184:114236. doi: 10.1016/j.addr.2022.114236. Epub 2022 Mar 26. PMID: 35351470; PMCID: PMC8957368.
Wong DWL, Klinkhammer BM, Djudjaj S, Villwock S, Timm MC, Buhl EM, Wucherpfennig S, Cacchi C, Braunschweig T, Knüchel-Clarke R, Jonigk D, Werlein C, Bülow RD, Dahl E, von Stillfried S, Boor P. Multisystemic Cellular Tropism of SARS-CoV-2 in Autopsies of COVID-19 Patients. Cells. 2021 Jul 27;10(8):1900. doi: 10.3390/cells10081900. PMID: 34440669; PMCID: PMC8394956.
Yonker LM, Swank Z, Bartsch YC, et al. Circulating Spike Protein Detected in Post–COVID-19 mRNA Vaccine Myocarditis. Circulation. 2023:147(11).